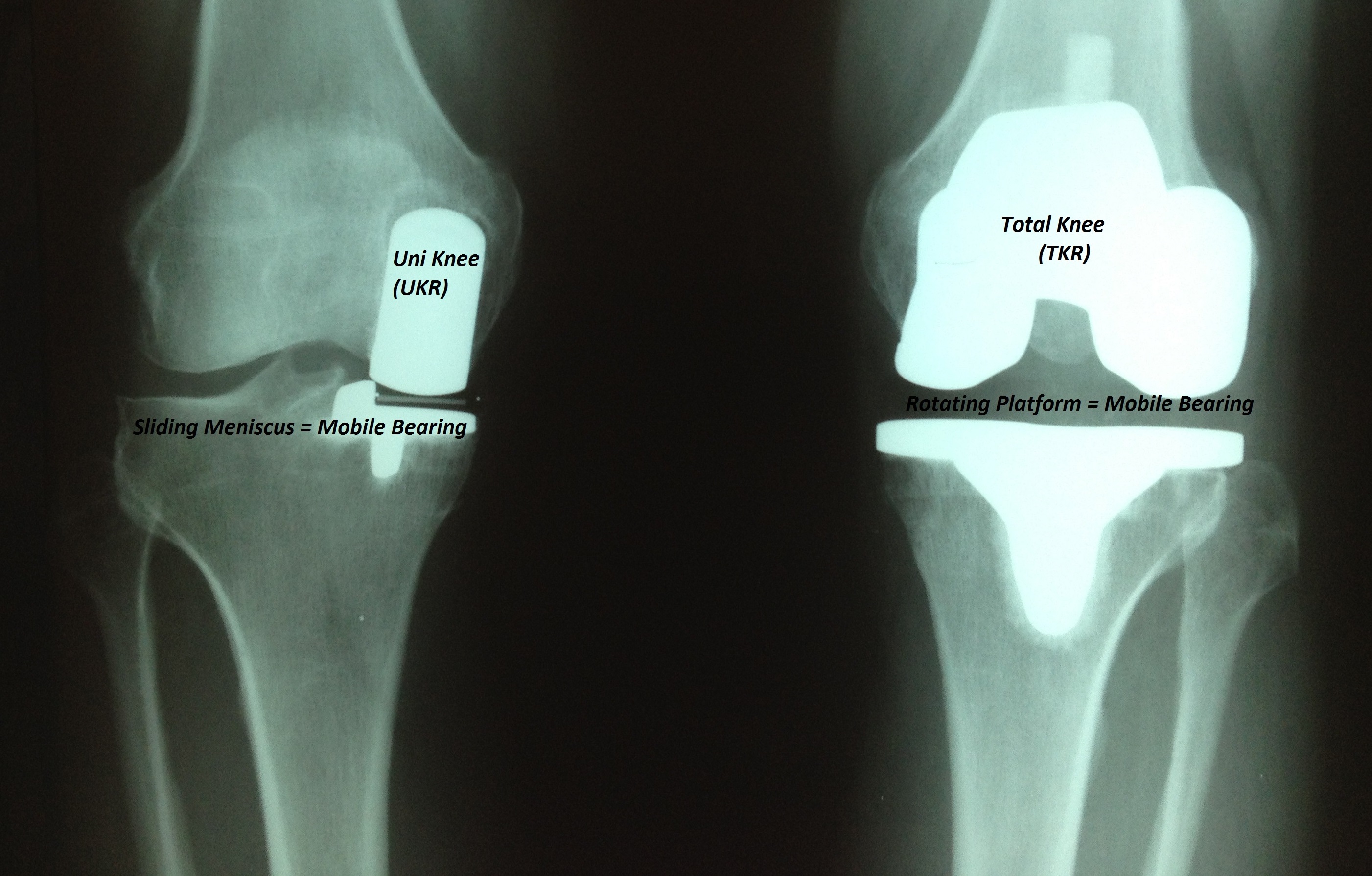
Many orthopedic surgeons who perform knee joint replacements are taking another look at Unicondylar Knee Replacements ( aka Partial Knee Replacement). Uni knees are designed with either a fixed bearing design or a mobile bearing design. Both designs have shown good success, and your surgeon will explain the type he prefers and why.
There are many reasons, but some include : improvement in biomaterials that can resist wear and tear over time – i.e., the plastic spacers that serve to substitute for the worn out meniscus ; the ability to use better pain-management protocols that facilitate early rehabilitation ( most patients can walk on their new partial knee immedicately after surgery ); out-patient facilities ( the rise of ambulatory surgery centers or ASCs) that can perform these partial knee replacements in the same day as discharge to home. Patients desire to return to work and athletic activities as soon as possible. The incision and muscle disruption is less compared to a “Total” Knee Replacement, so in general, recovery is faster. Typically, formal post-operative physical therapy is not required, although some patients choose to do it. A comprehensive home exercise program appears to give similar range of motion results over time. Lastly, studies that have compared the satisfaction of a total knee vs. a partial knee ( in the same patients ), hve shown a predilection to prefer the partial knee. The easiest way to explain this, is a partial knee does not remove many of the “normal structures” – such as the ACL ( anterior cruciate ligament, PCL (posterior cruciate ligament), lateral meniscus: structures that remain in the knee and continue to “transmit” neural feedback ( proprioception) to the brain – this feedback includes “positional sense”, that makes it more effective for athletes to “react” with reflexive action. Not all patients with knee arthritis are candidates for a partial knee. Talk to your knee surgeon to find out if you are a possible candidate for Unicondylar Knee Replacement.