Minimally Invasive & Muscle Sparing Total Joint Replacements Keep People Active Longer
Active people are living longer and are able to enjoy sports and physical activities well after their “sixties”. Orthopedic surgeons and their patients are enjoying increased success at replacing human joints with better and longer lasting implant technologies. Looking back, I have a good perspective on the state of the art in Joint Replacement, as I have been doing them for many years in a private practice in Scottsdale, Arizona. I am a Fellowship trained Total Joint specialist, having completed the additional training at Harvard Medical School, and I do not think that makes a difference when you look for a surgeon to replace your knee or hip. It is OK to ask your surgeon how many Total Hips or Total Knees he does a year. A good rule of thumb is to see someone who does over 100 of either (or both) when you choose to proceed. Super strong and light bio-materials such as titanium and Vitamin E impregnated polyethylene are helping patients with joint arthritis live a better and more active life. Most people over 50 know a friend or relative who has had a total hip or total knee replacement. Joint replacements are very successful at relieving severe pain and are now lasting many more years. With total techniques, the average 65 year old will not likely need a revision due to long term wear of a well done hip replacement using present day cementless technology by a fellowship trained total joint surgeon.

When I started orthopedic practice 26 years ago total knees had a history of lasting 12 to 15 years before the plastic wore out and a revision was needed. This was one reason we tried to elay surgery until the patient was older. Newer technologies and better understanding of techniques are improving the lifespan of modern joint replacements to 30 years and beyond. It is now possible to do these operations on younger, more active patients, and feel good about the long term prospects. Previous recommendations to avoid certain sports and labor are softening as we see patients with joint replacements doing better enjoying fast activities such as tennis, golf, and skiing. Most patients are satisfied to do hiking, fast walking, swimming, and bike riding, but others are choosing to do more. There are no studies on the results of patients who have done more extreme or strenuous sports. So far, I have not seen any correlation to an early failure rate.

One new technique you may hear about in knee replacement involves the use of a computerized navigation system to plan and more accurately execute the positioning of the implants. The hope was that the total knee computer would calculate a mathematical image of a patient’s leg and predict the best bone cuts to position the implants perfectly. Unfortunately, the input data points are chosen by the surgeon using his best “eye only” ability, and it turns out, the computer output data is no more accurate than the surgeons “eye” was in the first place. Given the expensive equipment and the added downside of drilling additional pin holes to obtain the data, the computer navigation is still not ready for “prime time. The public like “gizmos” and computers, so the idea persists and some surgeons use it as a marketing tool. The simple truth is, if it was better all surgeons would be using it. It is NOT better. So far the best we have is the well experienced surgeon’s brain, which is a remarkable computer in itself! I worked with the computer when it first became available, it turned out to be a big disappointment, and my results remain much better without it.

In the future, computer marking pins will be replaced with permanent electrode capsules, much like implantable chips that can be placed in pets to locate them if they are lost. The chips will transmit position data to the computer, and when combined with future “smart implants” will let the surgeon know if the implants are functioning normally. Patients with chip imbeded implants will get a check up by placing the leg under the “GPS” sensors, so the surgeon can “see” beneath the skin on his computer screen as the patient moves his knee. There is always room for improvement, and scientists and engineers continue to work on this project.
Other advances involve using less invasive “tissue sparing” approaches to the hip and knee joints. By limiting the soft tissue trauma as the implants are placed on the skeleton, the functional recovery is greatly accelerated. As the Medical Director of the Scottsdale Healthcare Total Joint Replacement Center on the Osborn campus, we have established a program that emphasizes very rapid recovery. All patients are encouraged to walk about 1 hour after their surgery is completed, full weight bearing unless there is an unusual circumstance. Total knee patients have their surgery with a pumping boot on the non-operative leg to keep blood circulating at all times, and we have seen a significant decrease in clotting problems. It appears that most of the risk related to blood clots in the veins is from immobility. So we get you up ASAP, and our deep venous thrombosis rate is way down (approx 1%). We do give you aspirin if you can take it as a blood thinner. High risk people for clotting are given Lovenox shots or coumadin pills. An example of a high risk patient is one who has had a clot once before after surgery, or one who has a hereditary clotting disorder like Leiden V factor deficiency.
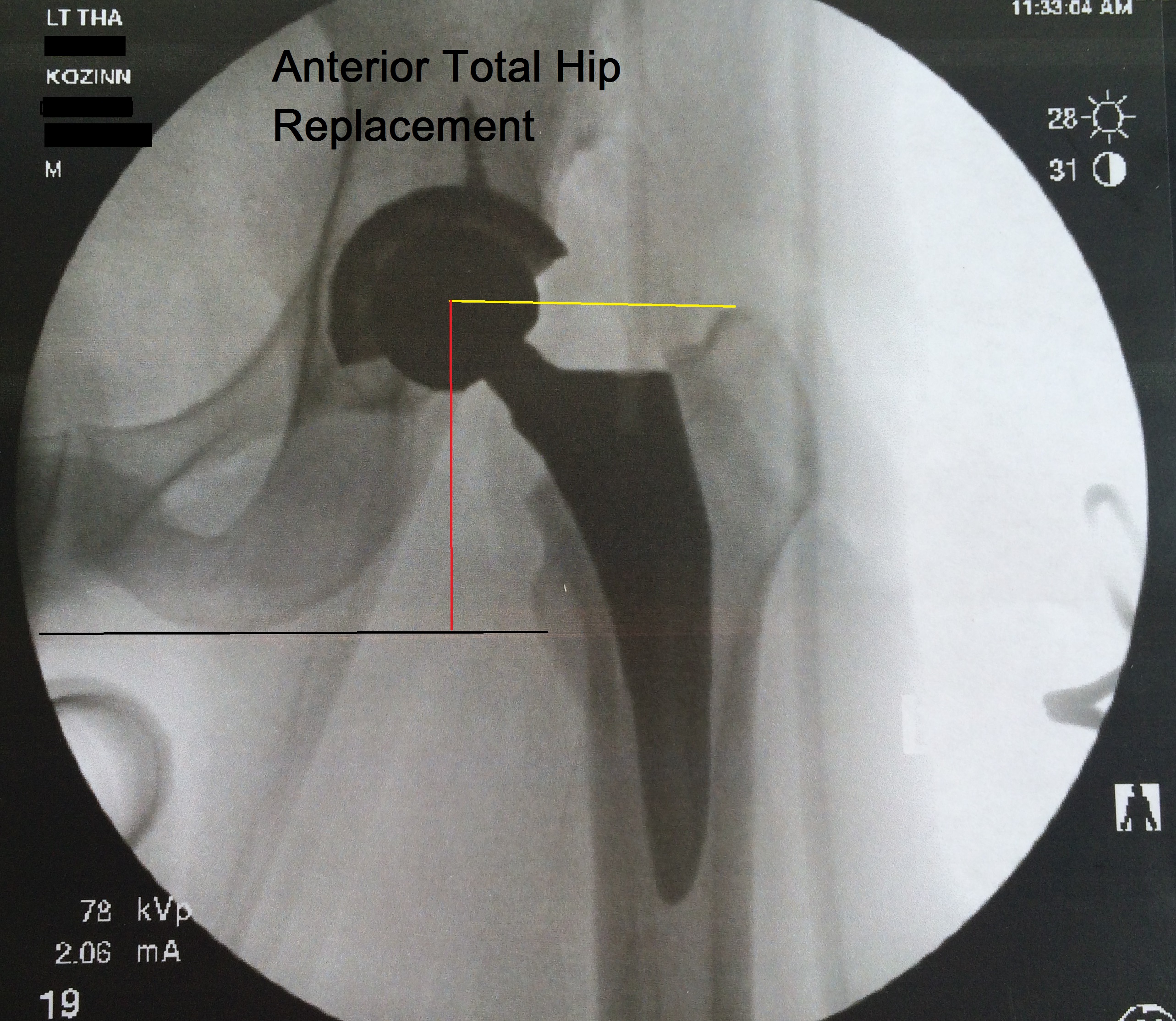
 The amazing anterior hip replacement technology is catching on throughout the nation. Dr. Kozinn is a recognized expert on this procedure. The hip replacement is done on a special table, and no muscles are cut on the approach to the hip. Pain is much less, and recovery is greatly accelerated. Dr. Kozinn is writing up a paper for publication of his series of outpatient total hip replacements. These are patients who had the anterior hip procedure and went home on the same day. Now that really is progress! The anterior hip patients are getting back to work and activities much faster than the other hip approaches. I believe this procedure will be the standard of care within the next few years.
The amazing anterior hip replacement technology is catching on throughout the nation. Dr. Kozinn is a recognized expert on this procedure. The hip replacement is done on a special table, and no muscles are cut on the approach to the hip. Pain is much less, and recovery is greatly accelerated. Dr. Kozinn is writing up a paper for publication of his series of outpatient total hip replacements. These are patients who had the anterior hip procedure and went home on the same day. Now that really is progress! The anterior hip patients are getting back to work and activities much faster than the other hip approaches. I believe this procedure will be the standard of care within the next few years.
Special multi-modality pain management protocols are now in effect at the Scottsdale Joint Center that speed up recovery. A femoral nerve block is used on all knee replacements to greatly decrease post op pain for 24hrs. We also favor spinal anesthesia, as it has been shown to be safer than general anesthesia and has added benifits of decreasing blood pressure, which decreases bleeding during the surgery. Also the venous dilation that occurs is associated with a decrease in the rate of deep venous thrombosis. You can still be “asleep”, but it is thru IV sedation, without all the drugs needed to paralyze and intubate. We de-emphasize morphine like drugs in the post-op period and use a number of non-narcotic medications along with simple Tylenol and Celebrex. IV Toradol is the mainstay of pain medications during the early post-op periord. Patients recover faster and better, when less narcotics are used.
 Total knee patients awake in the recovery room with no pain becasue the spinal anesthesia is still in effect. New techniques in “regional” anesthesia have decreased the pain associated with knee replacement surgery. The femoral nerve block greatly decreases the immediate pain upon waking up, yet still allows early ambulation. Patients need to be aware that the knee may buckle until the block wears off, so we are careful to prevent falls. Most of the total knee patients should accept the femoral nerve block as it helps speed up the recovery. At home most patients just take a few of the norco or vicoden thet we prescribe. Patients quickly get off the narcotic medications and use Motrin and their arthritis pill for pain relief.
Total knee patients awake in the recovery room with no pain becasue the spinal anesthesia is still in effect. New techniques in “regional” anesthesia have decreased the pain associated with knee replacement surgery. The femoral nerve block greatly decreases the immediate pain upon waking up, yet still allows early ambulation. Patients need to be aware that the knee may buckle until the block wears off, so we are careful to prevent falls. Most of the total knee patients should accept the femoral nerve block as it helps speed up the recovery. At home most patients just take a few of the norco or vicoden thet we prescribe. Patients quickly get off the narcotic medications and use Motrin and their arthritis pill for pain relief.
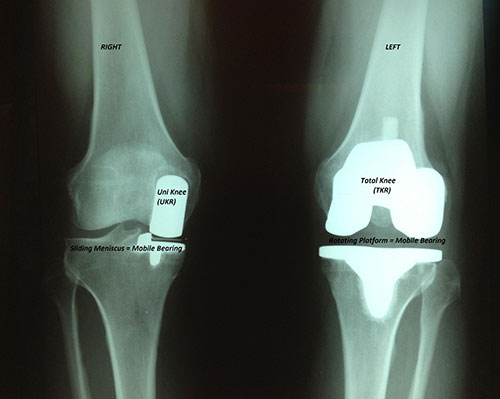
Knee implant designs are also improving, which will significantly increase the life span of total knees. I most often use a mobile bearing highly cross-linked polyethylene insert called a “rotating platform” in younger and more active patients. This allows a few degrees of twisting motion in the knees during sports such as tennis and golf, and acts as an additional shock absorber over the long term. I think the rotating platform knee is the single biggest advance in knee replacement design. My patients have been doing better since i started using it. They are definitely doing more sports and being more active, and I have less fear of plastic wear out.
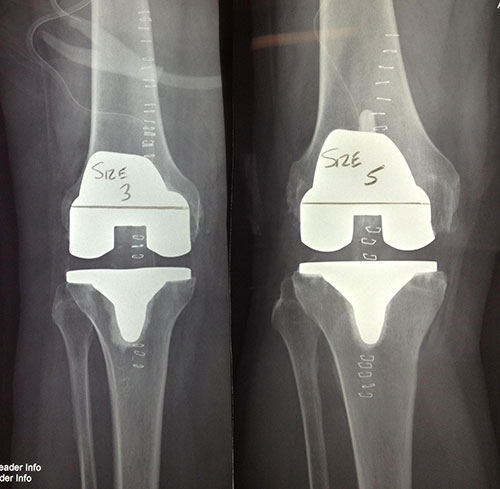
Total knees come in sizes, like shoes. Big knees get big implants, little knees get little implants. There is no need for a women’s knee, just a need for multiple sizes!
Partial knee replacements are very effective at relieving severe knee pain that is limited to one side of the joint. It is the only truly minimally invasive knee replacement. Smaller incisions and not muscle cutting leads to a more rapid recovery.. These are done through a very small incision that does not violate the quadriceps muscle, and recovery is very rapid. Patients with partial knees often go home after a one night stay in the hospital, and in most cases do not need formal physical therapy to regain their knee motion. The partial knee procedure is also less stressful on elderly patients and patients with significant heart or vascular disease. Range of motion is better, and the knee feels more like a normal knee. You must come in for an Xray to determine if you are a candidate for a partial knee.
 On the total hip side, new materials are likely to lead to longer lasting hips. High strength and light weight porous titanium implants encourage bone ingrowth creating a potentially permanent bond with the skeleton. Much improved bearing surfaces have been shown to last many more years before wearing down, and may never wear out in some patients. This includes ceramic materials, and very dense polyethylene plastic which in laboratory testing lasts many more years than earlier plastics. Larger diameter femoral heads are now routinely used to increase hip stability and range of motion. This allows patients to do more activities earlier, as the risk of hip dislocation is much less than it used to be with smaller diameter femoral heads. a new implant, the MDM3 is a bipolar device that greatly reduces the risk of dislocation. It does this by increasing the amount of hip motion available before impingement occurs. I like to use the MDM3 on revisions and difficult primary hips to decrease the risk of dislocation.
On the total hip side, new materials are likely to lead to longer lasting hips. High strength and light weight porous titanium implants encourage bone ingrowth creating a potentially permanent bond with the skeleton. Much improved bearing surfaces have been shown to last many more years before wearing down, and may never wear out in some patients. This includes ceramic materials, and very dense polyethylene plastic which in laboratory testing lasts many more years than earlier plastics. Larger diameter femoral heads are now routinely used to increase hip stability and range of motion. This allows patients to do more activities earlier, as the risk of hip dislocation is much less than it used to be with smaller diameter femoral heads. a new implant, the MDM3 is a bipolar device that greatly reduces the risk of dislocation. It does this by increasing the amount of hip motion available before impingement occurs. I like to use the MDM3 on revisions and difficult primary hips to decrease the risk of dislocation.
The bottom line is that younger patients are now better candidates for joint replacement surgery than in the past. Their implants should function better and last longer. More patients are choosing a joint replacement to get on with the most productive times of their life. It is a very fulfilling time for joint replacement surgeons, as we feel we have more tools to offer patients better and more long lasting results than ever before. For more general info on hip replacement, visit our American Academy of Orthopedic Surgeons website to read patient information on a variety of hip replacement issues : http://www.orthoinfo.org/topic.cfm?topic=A00377
Stuart Kozinn MD
Medical Director of the Scottsdale Center for Joint Replacement
And check out our Facebook page at Facebook.com/scottsdalejointcenter